LFD-200: Two Proven Breakthroughs
One Smarter Therapy
By combining the precision of ADCs with the proven efficacy of steroids, we are unlocking a new therapeutic class for autoimmune and inflammatory diseases
Glucocorticoids (GCs) are widely used to manage many acute and chronic inflammatory disorders, including asthma, rheumatoid arthritis, vasculitis, eczema, allergic reactions or anaphylaxis, inflammatory bowel diseases, leukemias and lymphomas.
Although effective, these drugs have many unwanted side effects. When steroids are administered, particularly at high doses or for extended periods, they remain in the body long enough to impact multiple organs and systems beyond their target.
Despite current therapies, such as the biologics and JAK inhibitors, there is still a high unmet need for new treatments. For example, 70-80% of patients with rheumatoid arthritis with inadequate response to methotrexate do not achieve an ACR70 response above 25% across multiple Disease-Modifying Anti-Rheumatic Drugs (DMARDs), according to a review of response rates from multiple publications. As a reference, high dose prednisone, a commonly prescribed GC, achieves up to a 50% ACR70 response.
Lifordi Immunotherapeutics is currently evaluating LFD-200, our first ADC, in a Phase 1 study and expects to have initial data by the end of 2026.
Using an ADC to deliver a potent steroid directly to immune cells would harness the effectiveness of steroids and avoid the off-target toxicity that has hampered their broader or longer-term use. While this ‘magic bullet’ is not an entirely new concept, the success of this approach lies in identifying the right target and establishing the right formulation that delivers an effective, safe, and convenient treatment for autoimmune and inflammatory diseases.
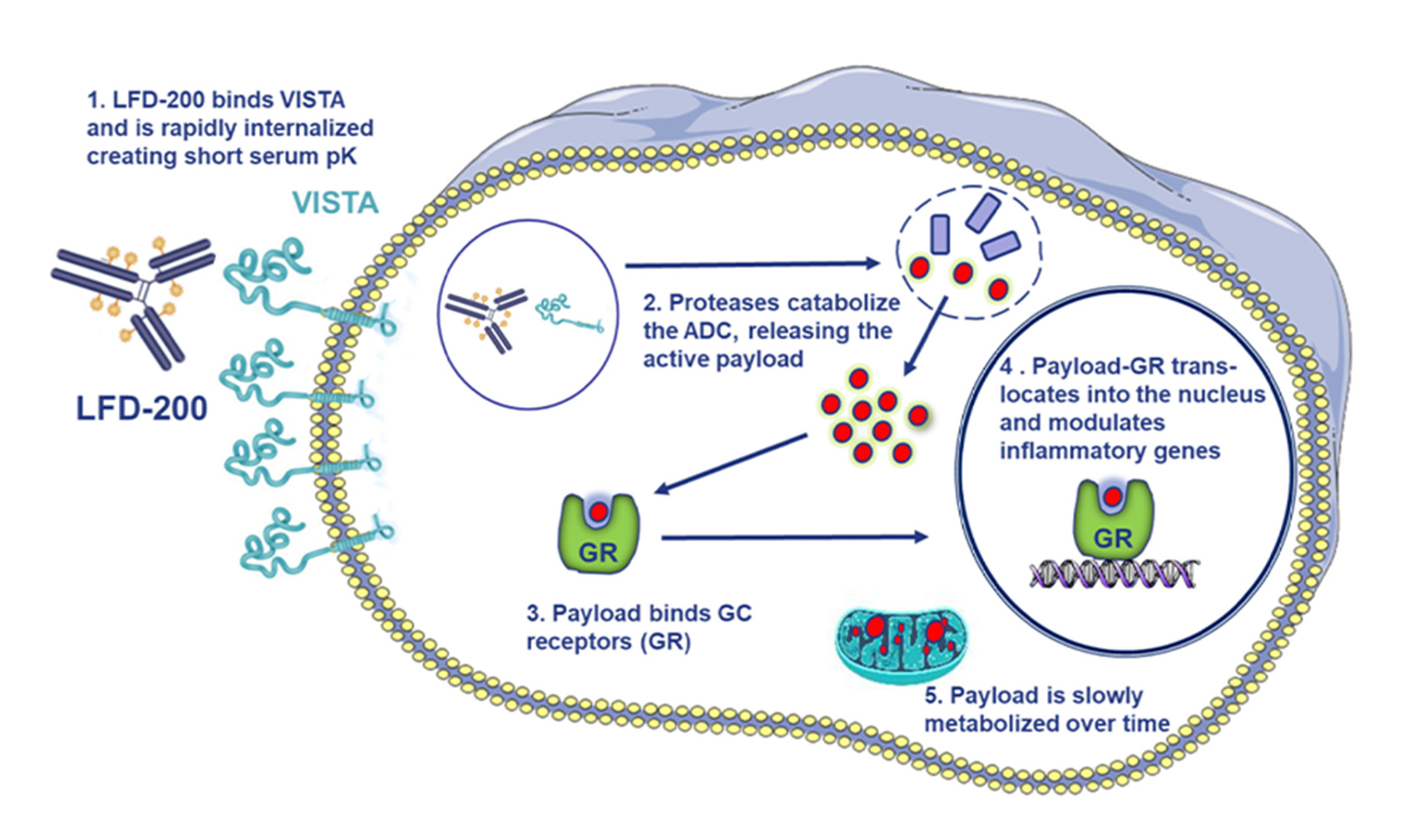
LFD-200 Mechanism of Action
LFD-200 is engineered to bind to VISTA, a cell surface protein selectively and highly expressed on immune cells, including myeloid, T cells and plasma B cells. Its unique properties, including its rapid internalization and accumulation of the drug payload, make it an ideal ADC target. A VISTA-directed ADC carrying a potent steroid demonstrated quick uptake by immune cells and a short serum half-life, measuring just hours vs. the days that is characteristic of serum residency for many ADCs. In other words, this ADC’s serum residency inside immunes cells far exceeds its exposure in serum.
As a result, there is much less concern that the ADC would be floating around in circulation for too long, potentially breaking off, releasing drug elsewhere in the body, and causing systemic toxicity.
LFD-200 Mechanism of Action
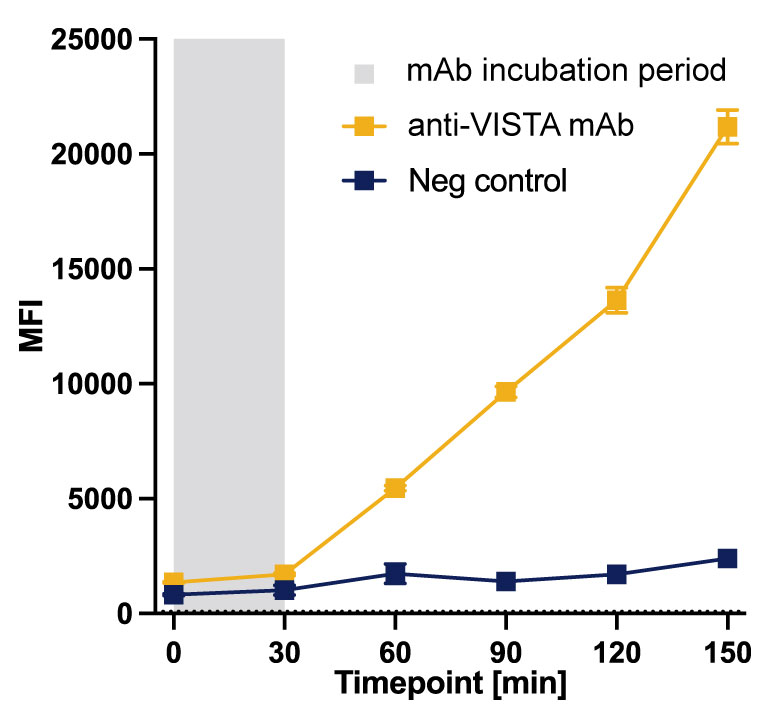
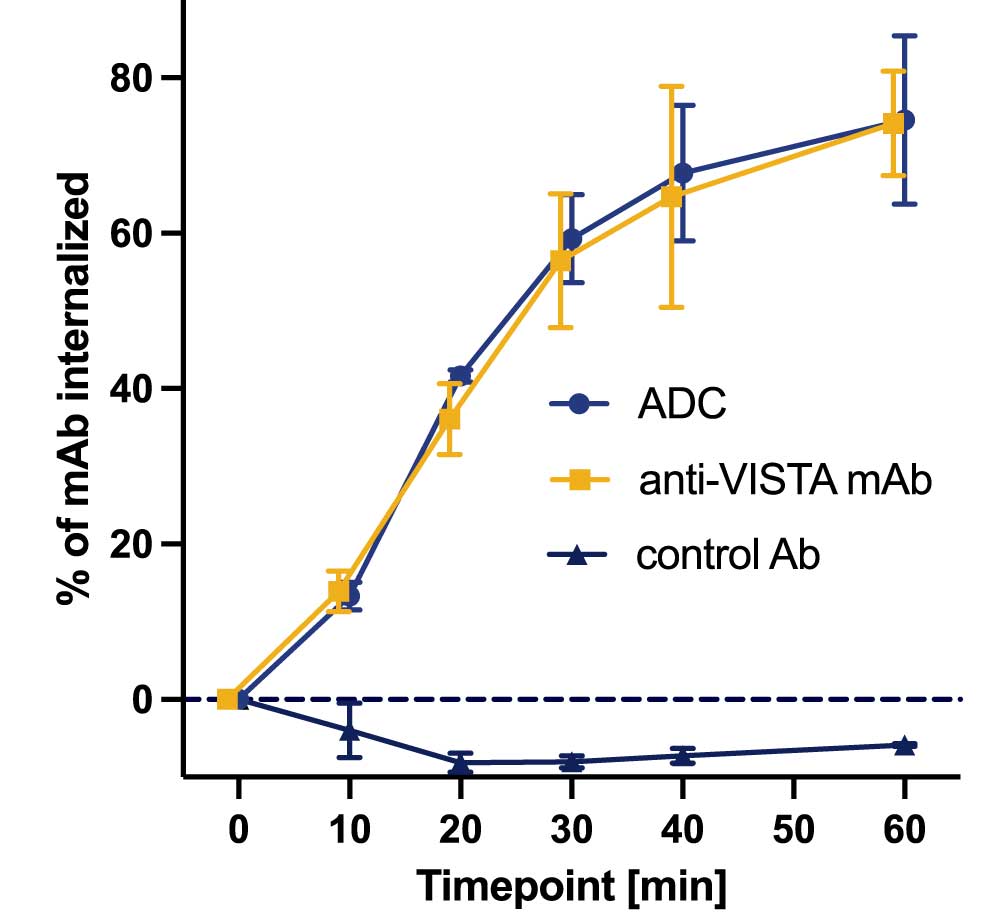
High Internalization with Lysosomal Accumulation in Human Monocytes
Short Serum Half Life with
Long Tissue Exposure*
LFD-200 Mechanism of Action
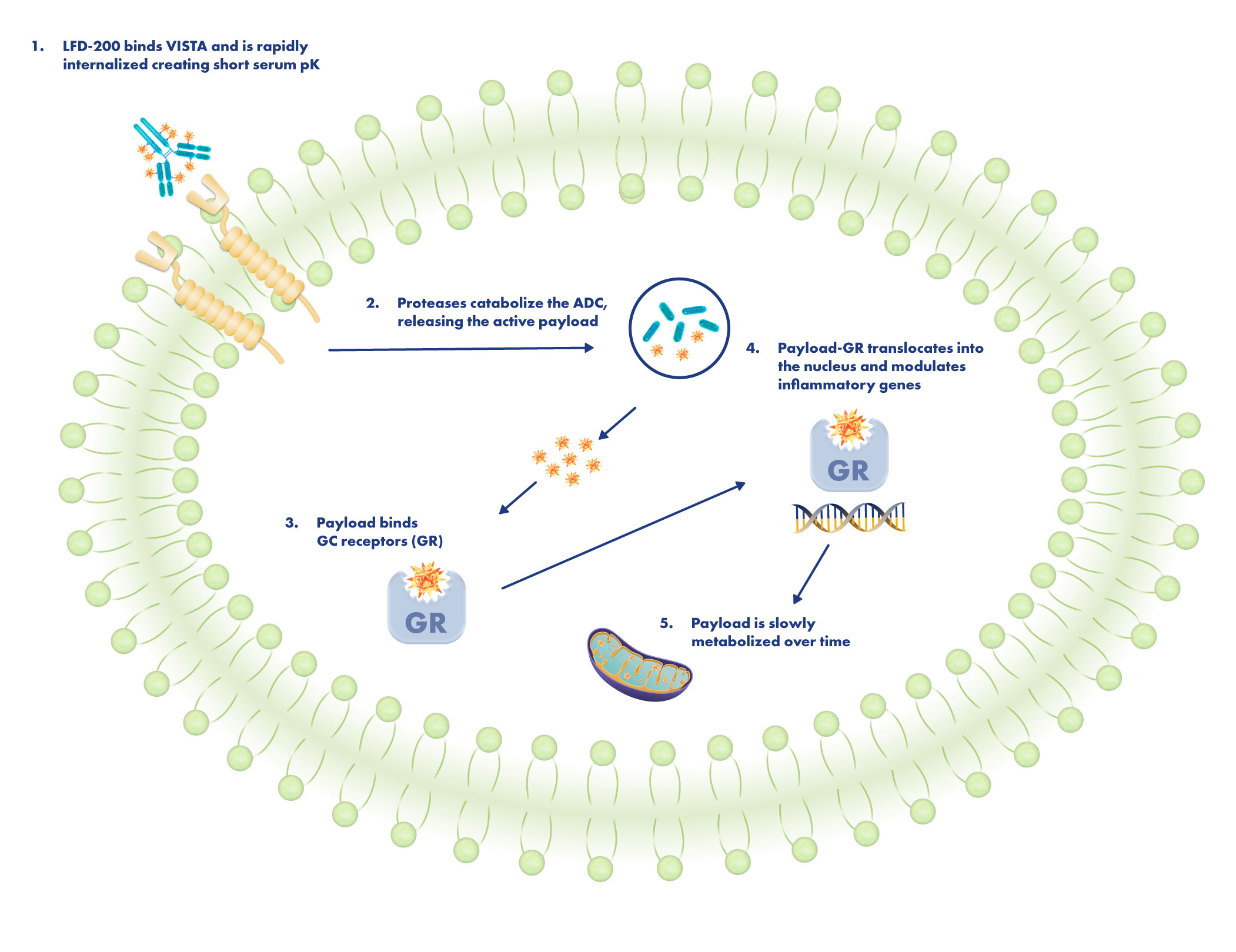
LFD-200 is designed to bind to VISTA, a cell surface protein selectively and highly expressed on immune cells, including myeloid, T cells, and plasma B cells. Its unique properties, including its rapid internalization and lysosomal accumulation, make it an ideal ADC target.
High Internalization with Lysosomal Accumulation in Human Monocytes
A VISTA-directed ADC carrying a potent steroid demonstrated quick uptake by immune cells and remains active in immune tissue for long periods. LFD-200’s short serum half-life measures just hours vs. the days or weeks that is characteristic of serum residency for many ADCs. In other words, this ADC’s residency inside immunes cells far exceeds its exposure in serum.
Short Serum Half Life with
Long Tissue Exposure*
LFD-200
Serum half-life = 14 hours
1 dose @ 10mg/kg
(delivers 0.2 mg/kg of Dex molar
equivalent payload)
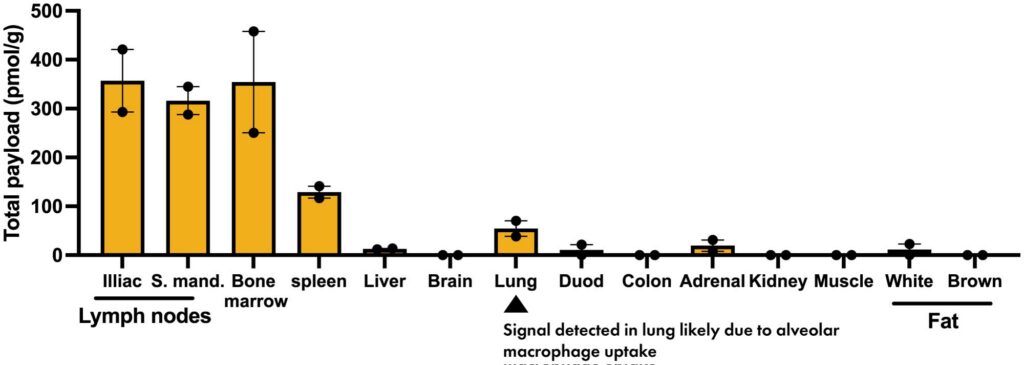
LFD-200 7 Days Post Injection
Dexamethasone:
Serum half-life = 2 hours
1 dose @ 2mg/kg
Dex 24h Post Injection
No preference for immune organ exposure
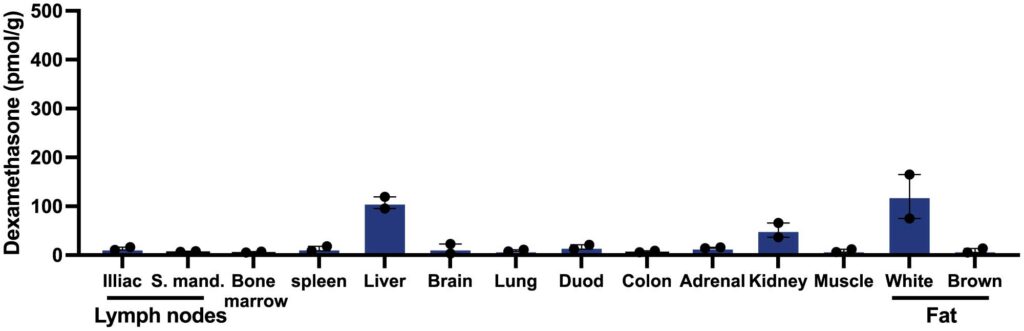
*In NHPs biodistrubution as measured by mass spetrometry (pmol of drug/gram of tissue). Comparative efficacious doses selected for LFD-200 and Dex; i.v. administration
As a result, there is much less concern that the ADC would be floating around in circulation for too long, potentially breaking off, releasing drug elsewhere in the body, and causing systemic toxicity. LFD-200 is delivered precisely to VISTA+ cells.
Preclinical studies of Lifordi’s lead ADC candidate, LFD-200, demonstrated a short serum half-life and long immune cell residency, as well as an ability to exert immunosuppressive function within these cells for an extended time without the toxicity associated with systemic delivery, as measured by no effect on cortisol levels – a highly sensitive measure of GC toxicity. Early data from clinical studies in healthy participants showed LFD-200 has a short serum half-life and long drug exposure, as well as the ability to suppress proinflammatory cytokines in an ex vivo functional model using whole blood samples.